In December of last year, the International OCD foundation (the leading authority on OCD and related disorders), conducted a study that was incredibly revealing to how frequently OCD is missed in an assessment. The study found that more than 75% of people living with OCD went undetected by healthcare providers. This adds context to why only 2% of individuals diagnosed with OCD actually receive Exposure and Response Prevention therapy, the gold standard of treatment for obsessive compulsive disorder.
One reason so many living with OCD go undetected by healthcare providers and therapists is because it’s wildly misunderstood. Media and online content often gives inaccurate depictions of the experience of living with OCD and it perpetuates false beliefs about this mental illness. Statements like, “I’m so OCD,” or “I let my intrusive thought win” when doing something you enjoy, is not at all what the lived experience of having OCD is like. Statements like this are minimizing, inaccurate, hurtful and perpetuate the misinformation on this disorder.
OCD is a doubting disorder. It is a disorder with intense fear, uncertainty, doubt and/or discomfort. Intrusive thoughts are egodystonic, meaning against our values and wishes, and thus someone with OCD would never joke about “letting their intrusive thoughts win”. In fact, letting their obsessive and intrusive thoughts “win” (acting on them), would be a nightmare. Some individuals with OCD compulsively respond to these intrusive thoughts with contingency plans to end their life or leave the country because of how distressing these thoughts are. The fear and discomfort of any of these thoughts coming true is so uncomfortable that some would rather imagine not living at all if it came true. I don’t mean to over-explain but I truly hope over time to help spread accurate information on this because it is so important to lead towards effective change.
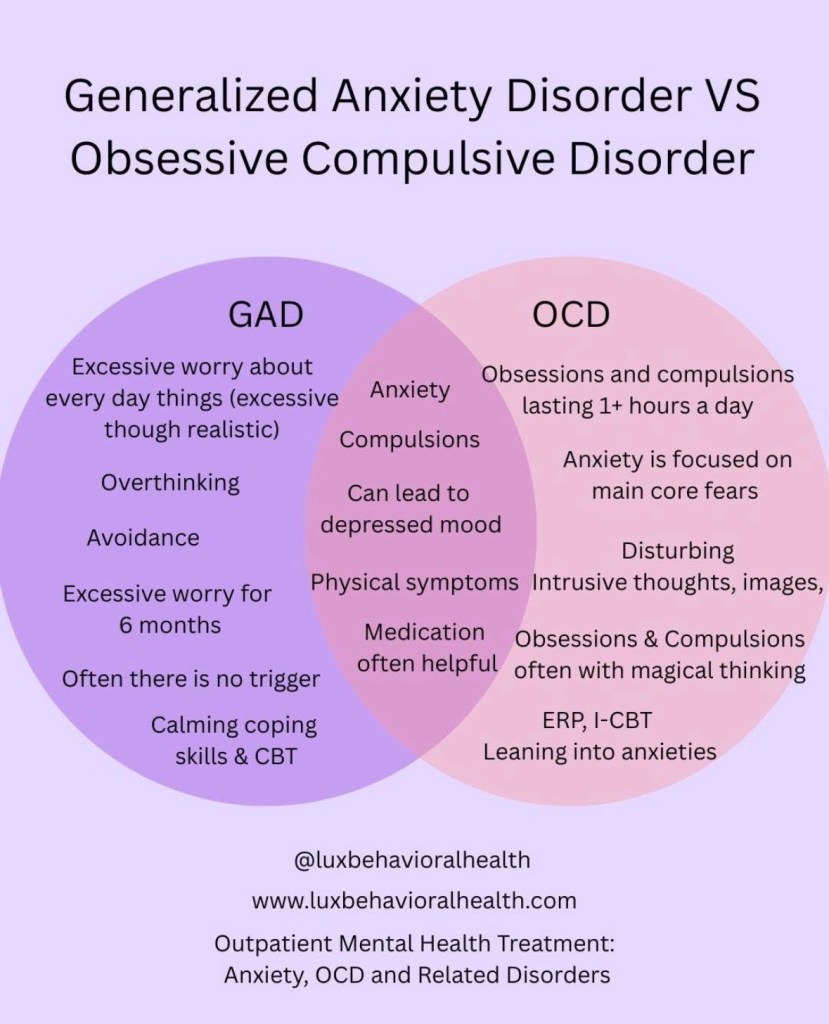
OCD can sound a bit like Generalized Anxiety Disorder (GAD) at times and so it is unfortunately common for clients to be diagnosed with GAD instead. Individuals with GAD tend to worry about every day, reality-based situations. There can be some compulsive behaviors like seeking reassurance or doing research (common in OCD as well) however with GAD, these actions actually work. The person does genuinely feel better and is able to let the worry go. Someone with OCD would only briefly feel relief before they need to continue to research or get reassurance.
There is limited time in graduate school to give a great deal of information about each mental health disorder. For this reason, there is an expectation of learning that happens for therapists while in the field. This is why fieldwork is required in order to graduate. Unfortunately, I’ve asked many therapists what was covered in grad school about OCD and the answers are very similar. The brief lesson on OCD tends to only cover “classic” and more obvious presentations of OCD like compulsive handwashing and compulsive checking. Working as an intern to complete fieldwork hours also doesn’t guarantee learning the nuances of each disorder. This leads to a gap such as this in accurate understanding of the disorder.
There are many individuals with OCD who do not have the presentation of compulsive handwashing or checking and there are many who don’t even have observable compulsions. Those with “pure ‘o’” OCD are those who only have mental compulsions and are most often the ones getting misdiagnosed.
I recently made a visual for our Lux Behavioral Health instagram page to highlight key differences and similarities with OCD and GAD. There is much more to it but I hope this visual is a helpful place to start.
I have so much passion for this work because I have lived experience with OCD. Unfortunately, part of this lived experience is being a statistic. What I mean by this is that because OCD is so misunderstood, it takes 14-17 years of treatment for someone to get an accurate diagnosis. I can relate to this and it is probably because I am someone who has mostly mental compulsions. I only was diagnosed after I figured it out myself! And even then I had to educate my providers as to why it was OCD and not GAD.
I hope this information is helpful and encourages readers to seek further education or deeper assessment. Even more so, I hope to bring awareness to those working in the healthcare field. The International OCD Foundation is calling this “America’s OCD Care Crisis” and based on the given statistics, crisis really is the appropriate word choice.
If you’re interested in reading this study please visit: America’s OCD Care Crisis – IOCDF Findings
Please reach out to us at Lux Behavioral Health if you have struggles with anxiety. We provide outpatient evidence-based therapy treatment in RI & MA and we are here to help!
